Intraoperative fluorescence is an invaluable tool in neurosurgery, with the first reported use of fluorescein for tumor resection dating back to 1948 by Moore (1). In the 1960s, the first applications in vascular neurosurgery were documented; however, technological limitations at the time prevented ideal results, and thus it was not widely utilized during that period (2, 3, 4, 5).
With technological advancements and a better understanding of fluorescence mechanisms, methods were developed to include light filters in microscopes, initially as independent setups, especially in Japan (6, 7, 8).
In 2005, Zeiss introduced the first fluorescence module integrated into a surgical microscope, bringing renewed attention to the topic and broader dissemination of similar technologies (9, 10).
In 2012, the launch of the first integrated fluorescence module with fluorescein greatly increased usage, being applied in vascular neurosurgery and guiding the resection of brain tumors.
This represented a significant milestone for neurosurgery; however, the technology was only available in the most advanced surgical microscopes, which typically have high prices ranging from USD 300,000 to USD 600,000, along with an additional fluorescence module cost exceeding USD 50,000.
During my neurosurgery residency at Santa Casa de São Paulo, I became interested in fluorescence. However, the technology was not – and still is not – widely adopted in Brazil, largely due to cost constraints. In 2016, I began exploring alternatives to make its use feasible within the context of our healthcare system. I studied how the modules work and, between 2016 and 2017, developed prototypes using light filters (Bandpass and Long Pass filters) with the same specifications as the commercial modules (16).
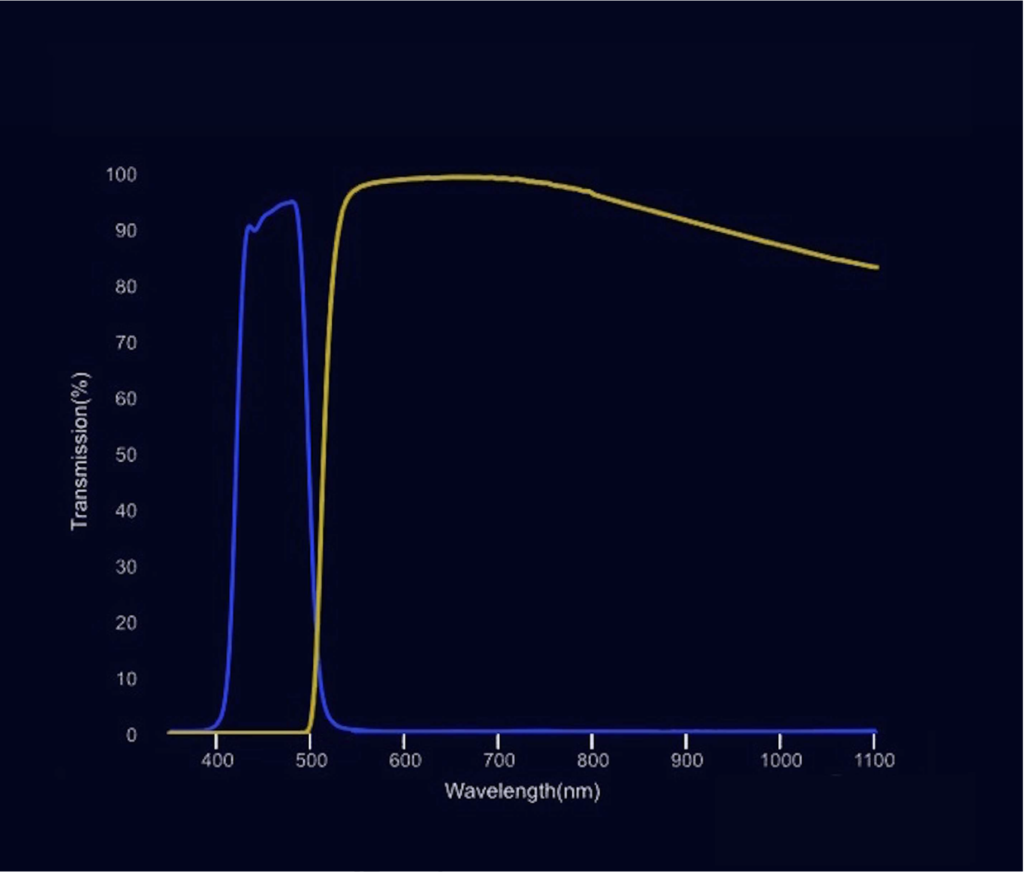
Fluorescein is an organic dye synthesized by Adolf von Baeyer that is widely and safely used in humans. It is a highly fluorescent molecule excited by light with a wavelength between 465 and 490 nm (blue) and has an emission peak between 520 and 530 nm (green). A blue light source and a yellow filter are necessary to properly visualize it, as will be described further. It is comparable to entering a room with a blue flashlight, illuminating the path while wearing glasses with yellow lenses.
The first functional prototype was built using the lens of the microscope’s sterile cover itself, a piece of EVA foam, and light filters positioned in the proper configuration for operation. Later, a 3D model was created for printing, allowing filters to be easily attached to the device. In 2017, the idea for the device was patented. Since then, I have assisted several neurosurgeons worldwide in using it during their surgeries. All project production costs, material sourcing, imports, and the INPI patent process were personally funded without any third-party financial support.

I believe the device’s concept is to make the technology accessible to everyone anywhere in the world. Therefore, I have decided to make the project available for free to anyone who wishes to use it, including files for 3D printing, ideal filter specifications, and basic building instructions.
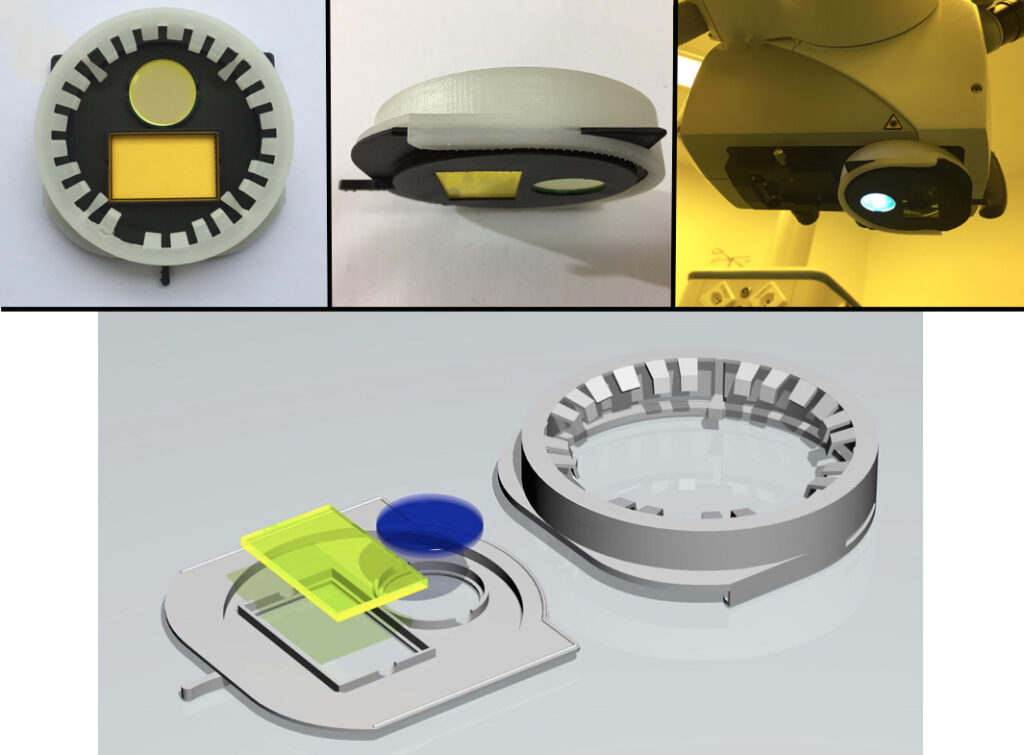
The device consists of an attachment to be coupled to the surgical microscope’s objective lens and a drawer-like holder for the filters, which can be inserted or removed during surgery as needed for fluorescence use (Downloadable files at the end of this page).
For ideal assembly, two filters are required: a round bandpass filter with a diameter of 25 mm to be placed in front of the light source, allowing light wavelengths between 460 and 490 nm (blue light) to pass through; and a longpass filter positioned in front of the microscope objective, permitting greenish light emission from the fluorescein while blocking blue light, resulting in a clearer image. I’ve also included a filter specification chart for easier purchasing worldwide.


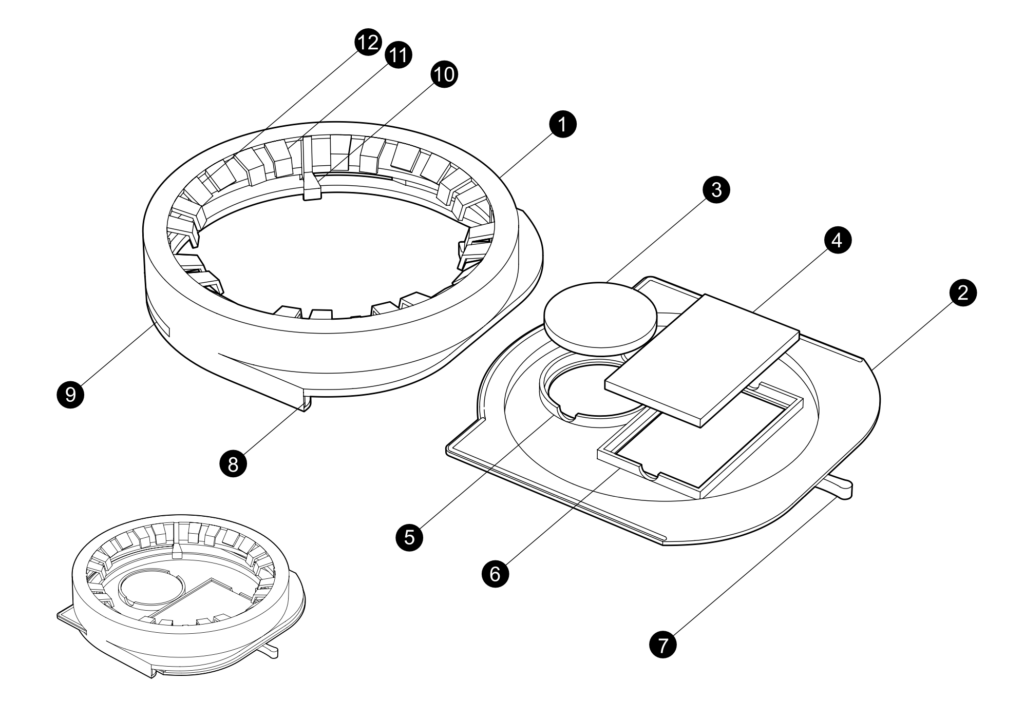
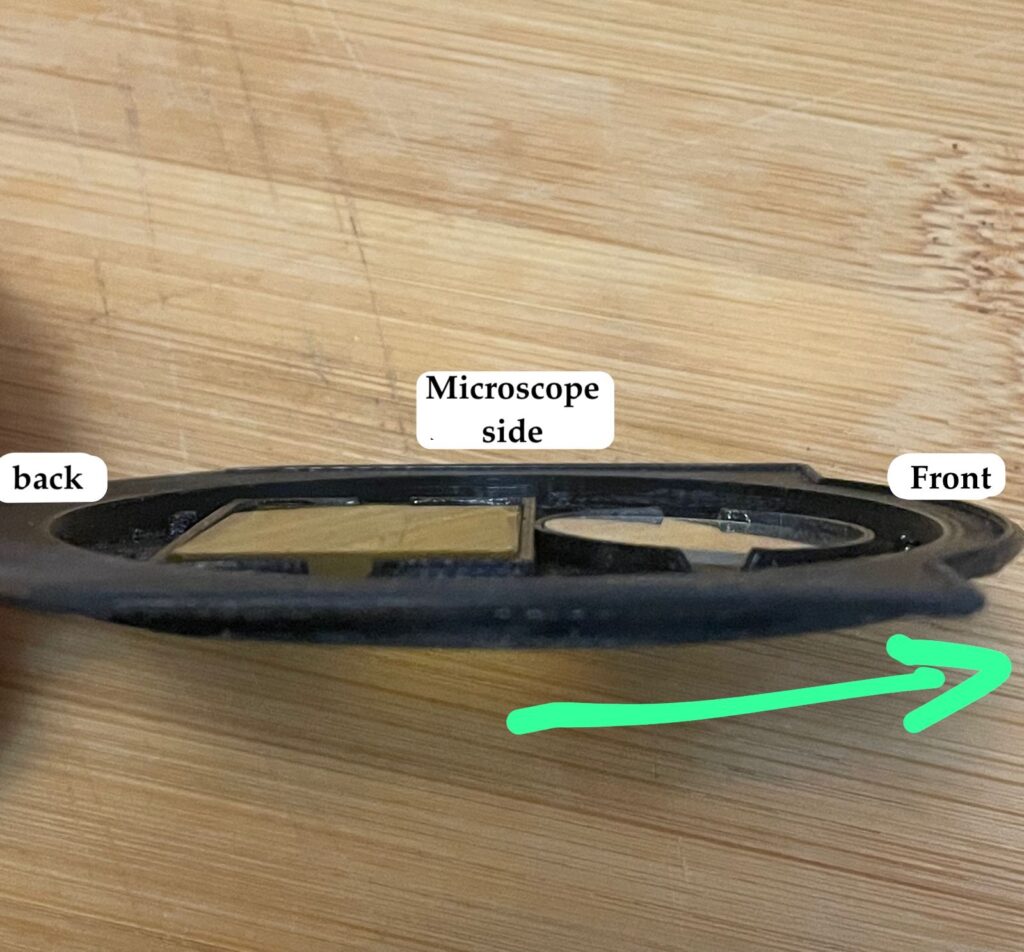
The filter-holder drawer is compatible with the microscope’s sterile cover. Thus, the portion of the device that attaches to the microscope does not need to be fabricated, as the sterile cover already includes a transparent lens that can be inserted or removed (in Figure 1, the blue section is the attachment that comes with the sterile cover and connects to the objective lens). This is the easiest way to use the device: simply print and build the filter-holder drawer and use the existing support on the sterile cover that attaches to the microscope.
Once the device is 3D-printed, sandpaper should be used to smooth its surfaces. Additionally, it may be necessary to sand the internal areas where the filters are inserted to ensure they fit in the correct position. The round filter should be perfectly parallel to the microscope or slightly angled forward, as shown in Figure 5. Otherwise, the mirrored surface of the bandpass filter angled backward could reflect light into the microscope’s objective lens, significantly impairing the image. Figure 6 schematically illustrates the device attached to the microscope and the drawer holding the filters.


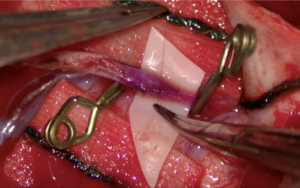
For brain tumor surgeries, the recommended dose of fluorescein is 3 to 5 mg/kg, administered intravenously before skin incision. This timing allows the fluorescein to accumulate in the lesion at areas where the blood-brain barrier is disrupted. To visualize the tumor, simply attach the device to the microscope and alternate between standard white light mode and fluorescence mode as needed.
For vascular neurosurgery, fluorescein serves a function similar to that of ICG (indocyanine green), enabling intraoperative video angiography. The recommended dose is 1 mg/kg, administered intravenously as follows: First, attach the device to the microscope and position the target arteries in the field of view. Then, bolus the fluorescein at the dosage described above, diluted in saline solution (0.9% NaCl) with a total volume of 15–20 mL. Approximately 20 seconds after administration, fluorescein becomes visible in the cerebral arteries.
If you use the device in your surgeries, I kindly ask you to document key moments with intraoperative images and videos or photographs. For brain tumors, it is important to note whether the lesion fluoresced and if the surgeon found the tool useful for the surgery, accompanied by pre- and postoperative images to evaluate resection extent. For aneurysms, verify that the aneurysm has no flow, check for residual neck involvement, and ensure the flow in surrounding arteries, perforating branches, and vessels remains intact. Confirm aneurysm occlusion postoperatively through imaging exams. Similarly, for cerebral revascularizations, immediate confirmation of anastomosis patency can be performed and verified postoperatively via CT angiography or cerebrovascular angiography. Documentation of such cases is encouraged, and I kindly request you to complete the questionnaire with case information. This will contribute to a database for evaluating the device’s utility, potentially supporting a future publication (using only aggregated data, without referencing specific cases) to promote broader adoption of the method worldwide.
Please feel free to use and widely share the link to ensure that everyone who wishes to use the device can do so without barriers.
The download for the device is FREE, along with absolutely unrestricted usage and distribution.
References: